|
ماذا تعرف عن ظاهرة لازاروس؟
مريض موت المخ المزعوم يتحرك ويظهر كافة مظاهر
الحياة .. فهو يحاول التنفس ويسعل ويحرك كافة
اطرافه واجزاء جسمه.
ظاهرة
لازاروس (راجع بحث اكذوبة موت المخ ):-
تعترف مراجع نقل الأعضاء صراحة
بأن أخطر العوائق التي واجهت أكذوبة (مــوت المخ )
منذ اختلاقها هو الحركة المستمرة التي يبديها
المرضى الذين أعلن الأطباء أنهم موتى مخياً
تمهيداً لانتزاع الأعضاء منهم.. حيث تمتد حركة
هؤلاء المرضى لتشمل تحريك الأيدي والأذرع والأكتاف
والأرجل والأقدام وأصابع اليدين والقدمين وتحريك
الجذع ومحاولة النهوض والمجاهدة للتنفس كما تشمل
العشرات من صور الحركة الأخرى .. ونظراً لتكرار
حدوثها في هؤلاء المرضى فقد أطلق عليها اسم ظاهرة
لازاروس
Lazarus phenomenon
.. ولازاروس هو اسم الرجل الذي أحياه السيد
المسيح كما ورد في العهد القديم.. ولذلك فقد اختار
الأطباء هذا الاسم لإطلاقه على المريض الذي تم
تشخيصه بأنه ميت مخياًَ ولكنه يتحرك ويظهر مظاهر
وعلامات الحياة !!
ظاهرة لازاروس تسبب ترويع الأهل والأطباء على
السواء:-
تصف بعض المراجع ظاهرة لازاروس بأنها أكثر علامات
مرضى موت المخ ترويعاً
most startling .. إذ أن
الأهل والأطباء على السواء يشاهدون أمامهم إنساناً
يتحرك حركةً مركبةً وهادفةً وتلقائيةً
complex
& spontaneous
,
purposeful حيث يحاول القيام والنهوض
والتشبث بالحياة ولكن
أطباء نقل الأعضاء
يعلنون أنه ( ميت ) ويتأهبون لانتزاع أعضائه!
ظاهرة لازاروس
§
هذه الظاهرة واسعة الانتشار حيث تحدث في 70 – 75 %
من الحالات.
§
تظهر هذه الظاهرة في أشد صورها عند انتزاع أجهزة
التنفس الصناعي من المريض أثناء مايعرف باختبار (
وقف التنفس ) حيث قد يتحرك المريض فيحاول الإمساك
بجهاز التنفس الصناعي الذي ينزع منه كما لو كان (
ُيجاهد للتنفس
struggling to breathe
) وقد يحرك ذراعيه ورجليه ويحاول القيام من الفراش.
§
تأخذ الكثير من الحركات العضلية في ظاهرة لازاروس
شكلاً متكاملاً مثل إمساك اليدين ببعضهما أو تحريك
الرجلين بما يشبه المشي أو تحريك اليدين نحو
الكتفين أو تحت الذقن وتقاطعهما بشكل مقصود ولذلك
تصنف هذه الحركات على أنها ( مركبة وهادفة ).
·
لاتقتصر حدوث ظاهرة لازاروس على حالة خفض
الأكسجين بالدم أثناء إجراء ( اختبار وقف التنفس )
وإنما قد تحدث تلقائياً بدون مؤثرات خارجية كما
تحدث في بعض الحالات عند إحداث الألم أو وجود
مؤثرات حسية.
·
قد تستمر الحركة العضلية لعدة دقائق زادت عن
ثلاث دقائق ونصف في بعض الحالات تم تسجيلها
بالفيديو.
·
لاتقتصر ظاهرة لازاروس على حركة العضلات
للأطراف أو الرأس والكتفين وأصابع القدمين واليدين
وغيرها وإنما تمتد إلى الكثير من مظاهر الحياة
الأخرى مثل :-
1.
الكحة.
2.
إستمرار التنفس التلقائي ( متقطع وخفيف) (وتنفس متقطع )
لفترة قصيرة بعد نزع جهاز التنفس الصناعي.
Rhythmic shallow irregular respiratory activity
3.
تحريك الرأس من جهة إلى أخرى.
4.
موجات متكررة من الارتعاشات بأصابع اليدين
والتقلصات بالفك وعضلات الوجه تستمر لعدة
ثوانٍ.
الرد بالوثائق على مزاعم بعض الأطباء بأن ظاهرة
لازاروس هي أفعال انعكاسية تنشأ من الحبل العصبي
..
تؤكد المقالات الطبية الحديثة الواردة في الصفحات
القادمة أن أنواع وصور هذه الحركة أوسع كثيراً
مما كان يعتقد من قبل وأنها تتضمن أنواعاً من
الحركة يصعب وضعها تحت حصر أو تقسيم
(difficult to classify)..وأن
الكثير من هذه الحركات يتم في خطوات متتابعة
sequence of movements
ولتحقيق
هدف محدد..
purposeful
ولذلك فإنه لم يعد مقبولاً
ماكان أطباء نقل الأعضاء يرددونه من قبل تبريراً
لحركة مرضى موت المخ من أنها (
مجرد أفعال انعكاسية
spinal reflexes
صادرة من الحبل العصبي لا من المخ ) .. وقد اعترف
معهد الأعصاب الأمريكي في نيويورك في
دراسة له عام 2005 بغموض المنشأ والأسباب التي
تكمن وراء حركة هؤلاء المرضىpathophysiology
remains speculative
..واقترح في ختام
دراسته إطلاق تسمية جديدة تعبر عن هذا
الغموض حيث اقترح أن تسمى هذه الحركة
)
الحركة الذاتية المصاحبة لموتى المخ(
brain
death associated automatism
وهو اعتراف بسقوط كل المزاعم السابقة التي كان
الأطباء يسوقونها تبريراً لحركة هؤلاء المرضى ..
كما أنه اعتراف بسقوط مفهوم ( موت المخ ) ذاته إذ
لايعقل أن تتواجد حركة ذاتية
automatism
في إنسان
ميت!!
ظاهرة لازاروس في مريضة موت مخ عمرها 30 سنة
الصورة
A
الجسم في وضع الارتخاء
الصورة
B
الكوع الأيسر يدور ويقترب الذراع الأيسر من الجسم
الصورة
D
الذراعان يتحركان عند الضغط على
الكتف الأيسر
المصدر : مجلة الأعصاب الأمريكية
NEUROLOGY 2000;
54:224–227
حالة موت مخ – طفل عمره 11 شهر
|
C |
|
A
|
| |
|
|
الصورة
A
الجسم في وضع الارتخاء
الصورة
C
الكوع الأيسر يدور للداخل والذراع يقترب من الجسم
نفس الطفل يمسك بيد الطبيب عند إحساسه بها حتى أن
الطبيب يحاول بصعوبة استخراج يده من يد الطفل
الممسك به
المصدر : مجلة الأعصاب الأمريكية
NEUROLOGY 2000;
54:224–227
|
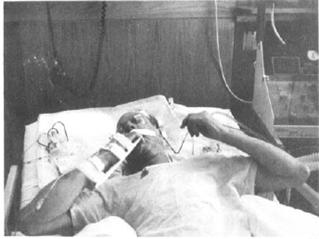
صور لمريض موت مخ ( مجلة الأعصاب
الأمريكية ) |
قبل نزع جهاز التنفس الصناعي من المريض
( الذراعين بجوار الجسم ) |
بعد 6 دقائق من انتزاع جهاز التنفس
الصناعي من المريض
( المريض يظهر علامات الحياة فيحرك ذراعيه
معاً إلى أعلى صدره) |
|
1
|
2
|
بعد 5 ثوان تالية
الذراعان
يتحركان أكثر نحو الفم وكأن المريض يجاهد
لمحاولة التنفس
(struggling to breathe) |
بعد 5 ثوان أخرى
(
الذراعان يلتقيان والأصابع تتشابك
أسفل الذقن) |
|
3
|
4

|
المصدر : مجلة الأعصاب الأمريكية
NEUROLOGY
1984;
34:1089
ظاهرة لازاروس في مريضة موت مخ
يابانية عمرها 43 سنة أثناء نزع جهاز التنفس
الصناعي

المريضة ترفع الذراع الأيمن وتفرد أصابع
اليد اليمنى |

المريضة ترفع الذراع الأيسر إلى أعلى
وتحرك الذراع والكف الأيمن نحو الفم |
Department of
Anesthesiology & Critical Care Medicine,
Ajou University
Hospital
صور المراجع والمجلات الطبية العالمية عن ظاهرة
لازاروس
Neurocritical care
Neurocrit
Care.2005,3(2):122-6
Brain death-associated
reflexes and automatisms
Samay Jain1 and
Michael DeGeorgia2
|
Division of Movement
Disorders, Neurological Institute,
710 W. 168th St., 3rd Floor,
10032 New York, NY |
(1) |
|
Department of
Neurology and Neurosurgery, The
Cleveland Clinic Foundation,
Cleveland, OH |
(2) |
Abstract Background: In
several instances,
the diagnosis of brain death has been questioned
due to the presence of movements.
This case report and review of the
literature illustrates the spectrum of movements
that have been encountered in brain death.
Methods: A case report and
review of the literature on movements seen in
brain death was conducted.
Results:
Movements in
brain death are common and have a wide range of
phenomenology. Several movements wax and wane
over time, making movements in brain death
difficult to classify.
In addition, varying terminology has been
used (e.g., Lazarus sign, spinal man, spinal
reflexes, spinal automatisms). Although evidence
points to a spinal origin for such movements,
the pathophysiology in many cases remains
speculative. Characteristics of movements in
brain death have been identified that can help
differentiate them from brainstem or voluntary
origin.
Conclusions: Based on our
review, we suggest referring to
stimulus-provoked movements as reflexes and
spontaneous movements as automatisms.
We propose
using the terms brain death-associated reflexes
and brain death-associated automatisms as
two main categories for movements that occur in
brain death.
These terms do not imply a specific
pathophysiology, but consistent
clinically oriented nomenclature may be useful
when reporting such phenomena.
__________________________________________________________
European Journal of
Neurology

Eur J Neurol.
2004 Nov;11(11):723-7.
Undulating
toe movements in brain death
Saposnik G,
Mauriño J,
Saizar R,
Bueri JA.
Movements in Brain Death Study Group, Department of
Neurology, Hospital JM Ramos Mejía, Universidad
de Buenos Aires, Buenos Aires, Argentina.
gsaposnik@yahoo.com
For many years, death
implied immobility. Nevertheless, there are
anecdotal reports of spontaneous or reflex
movements (SRMs) in patients with Brain death
(BD). The presence of some movements can
preclude the diagnosis of BD, and consequently,
the possibility of organ donation for
transplantation.
McNair and Meador [(1992), Mov Dord7:
345-347] described the presence of undulating
toe flexion movements (UTF) in BD patients.
UTF consists in a sequential brief plantar
flexion of the toes. Our aim was to determine
the frequency, characteristics and predisposing
factors of UTF movements in a prospective
multicenter cohort study of patients with BD.
Patients with confirmed diagnosis of BD were
assessed to evaluate the presence of UTF using a
standardized protocol. All patients had a
routine laboratory evaluation, CT scan of the
head, and EEG. Demographic, clinical,
hemodynamic and blood gas concentration factors
were analyzed. amongst 107 BD patients who
fulfilled the AAN requirements, 47 patients
(44%) had abnormal movements. UTF was observed
in 25 (23%) being the most common movement
(53%). Early evaluation (OR 4.3, CI95% 1.5-11.9)
was a predictor of UTF in a multivariate
regression model. The somato-sensory evoked
potential (SSEPs) as well as brainstem auditory
evoked potentials (BAEPs) did not elicit a
cortical response in studied patients with UTF.
This spinal reflex is probably integrated in the
L5 and S1 segments of the spinal cord. Abnormal
movements are common in BD, being present in
more than 40% of individuals. UTF was the most
common spinal reflex. In our sample, early
evaluation was a predictor of UTF. Health care
professionals, especially those involved in
organ procurement for transplantation, must be
aware of this sign. The presence of this motor
phenomenon does not preclude the diagnosis of
BD.
__________________________________________________________
Transplantation
Proceedings

Transplant
Proc.2004 Jan-Feb,36(1):17-9
Frequency of spinal
reflex movements in brain-dead patients
Authors:
Dosemeci L.1; Cengiz
M.; Yilmaz M.; Ramazanoglu A.
Spontaneous and reflex
movements may occur in brain-dead patients.
These movements originate from spinal cord
neurons and do not preclude a brain-death
diagnosis. In this study, we sought
to determine
the frequency and characteristics of motor
movements in patients who fulfilled diagnostic
criteria for brain death. Patients
admitted to our department between January 2000
and March 2003 and diagnosed as brain-dead were
prospectively evaluated in terms of spinal
reflexes. Clinical brain death was diagnosed
according to our national law. We also prefer to
document the diagnosis of brain death with an
EEG and/or TCD. Spinal reflex movements were
observed in 18 out of 134 (13.4%) brain-dead
patients during the study period.
Lazarus sign,
the most dramatic and complex movement seen in
brain-dead patients, was observed a
few times in two patients during an apnea test,
an oculocephalic test, after a painful stimulus,
and after removal of a ventilator. The other
reflex movements observed in our
brain-dead
patients were finger and toe jerks, extension at
arms and shoulders, and flexion of arms and
feet. The occurrence of spinal reflexes in
brain-dead patients may certainly delay decision
making, such as starting a transplantation
procedure, because of difficulties in convincing
the family or even a physician taking part in
the diagnosis of brain death. An
awareness of spinal reflexes may prevent delays
in and misinterpretations of the brain-death
diagnosis
__________________________________________________________

Acta Neurol Scand. 2003
Sep,108(3):170-3
Complex spinal reflexes
during transcranial Doppler ultrasound
examination for the confirmation of brain death
Authors:
de Freitas, G. R.1; Lima, M. A. S. D.1; André,
C.1
Abstract:
De Freitas GR,
Lima MASD, André C. Complex spinal reflexes
during transcranial Doppler ultrasound
examination for the confirmation of brain death.
Acta Neurol Scand 2003: 108:
170-173. © Blackwell Munksgaard 2003. Objective
Complex sets of movements of
the extremities can be seen in patients with
brain death (BD), and are typically observed
during apnea testing or removal of ventilatory
support (also called the Lazarus sign). We here
describe brain-dead patients who had not shown
previous movements, even during apnea testing,
but presented complex spinal reflexes during
transcranial Doppler (TCD) examination elicited
by neck flexion. Methods -
We performed a prospective
TCD study of patients with the clinical
diagnosis of BD. Results -
Four (2.5%) of
161 brain-dead
patients presented complex spinal reflexes
exclusively during TCD examination.
TCD showed vertebro-basilar circulatory arrest
in all four. Their systolic blood pressure was
significantly lower than that of brain-dead
patients not presenting movements during TCD
examination.
Conclusions :Hypotension and mechanical
stimulation play a role in the pathophysiology
of complex spinal reflexes present in BD, which
are not exclusively seen in terminal hypoxia.
Intensive care personnel and neurologists who
perform TCD to confirm BD should be aware of
these movements.
__________________________________________________________
Journal of the American
Academy of Neurology
Neurology 2000,54:221
Spontaneous
Movements Often Occur After Brain Death
Science Daily
—
ST. PAUL,
MN - Many
brain-dead patients have spontaneous movements
such as jerking of fingers or bending of toes
that can be disturbing to family members and
health care professionals and even cause them to
question the brain-death diagnosis.
These movements occur in 39 percent of
brain-dead patients, according to a study
published in the January 11 issue of Neurology,
the scientific journal of the American Academy
of Neurology.
"We found that these movements are more common
than has been reported or believed,"
said neurologist and study author José Bueri,
MD, of J. M. Ramos Mejia Hospital in Buenos
Aires, Argentina. "People need to know that
these movements are spinal reflexes that do not
involve any brain activity."
The study
examined all patients at the hospital during an
18-month period with a diagnosis of brain death.
Of the 38 patients, 15 had these motor
movements. In all cases, the movements were seen
in the first 24 hours after brain death
diagnosis, and no movements were seen after 72
hours.
Some of the
movements occurred spontaneously; others were
triggered by touch. Examiners used tests
designed to elicit motor movements, such as
lifting the arms or legs or touching the palm of
the hand.
Electroencephalogram (EEG) tests did not show
any brain activity in any of the patients with
movements.
"If the lack of
understanding of these movements leads to a
delay in the brain death diagnosis or questions
about the diagnosis afterwards, there can be
important practical and legal implications,
especially for organ procurement for
transplantation," Bueri said. "Family members
and others need to understand that these
movements originate in the spinal cord, not in
the brain, and their presence does not mean that
there is brain activity.
One of the most startling movements for family
members and health care professionals is called
the 'Lazarus sign.' It is a sequence of
movements lasting for a few seconds that can
occur in some brain dead patients, either
spontaneously or right after the ventilator is
disconnected," Bueri said. It is named for the
episode in the Bible where Lazarus is raised
from the dead.
"It starts with stretching of the arms, followed
by crossing or touching of the arms on the
chest, and finally falling of the arms alongside
the torso," he said. "It is also a spinal
reflex, but it can be disturbing to family
members and others who see this."
Another article
in this issue of Neurology describes unusual
movements in two brain dead patients. The
movements occurred in a 30-year-old woman and an
11-month-old baby at a hospital in Barcelona,
Spain. Both
patients
extended
their arms,
flexed their wrists and curled up their fingers
each time the mechanical ventilator inflated
their lungs. The
movements
stopped after the patients were disconnected
from the ventilator.
"We had never seen these type of movements
before, and they hadn't been reported in the
medical journals," said neurologist Joan
Martí-Fàbregas, MD, PhD, of the Hospital de la
Santa Creu i Sant Pau.
The doctors
conducted additional tests and confirmed that
there was no brain activity. "The living cells
that were ordering these muscles to move were
not brain cells or brain stem cells, but cells
located in the spinal cord," he said. "It's
important for family members and health care
professionals to be aware of this possibility."
A neurologist is
a medical doctor with specialized training in
diagnosing, treating and managing disorders of
the brain and nervous system.
The American Academy of
Neurology, an association of more than 16,000
neurologists and neuroscience professionals, is
dedicated to improving patient care through
education and research .
__________________________________________________________
The American
Journal of Medicine
Volume 118, Issue 3, March
2005, Pages 311-314
Spontaneous
and reflex movements in brain death
G. Saposnik, MD, J. A.
Bueri, MD, J. Mauriño, MD, R. Saizar, MD and N.
S. Garretto, MD
From the Department of
Neurology, Hospital J.M. Ramos Mejía, Buenos
Aires, Argentina.
Address correspondence and
reprint requests to Dr. José A. Bueri,
Department of Neurology, Hospital J.M. Ramos
Mejía, Urquiza 609, Buenos Aires (1221),
Argentina.
Spontaneous and reflex movements may be found in
patients with brain death (BD). The
authors prospectively evaluated their
frequency using a standardized protocol. Among
38 patients who fulfilled criteria
for BD, the authors found 15 (39%) with
spontaneous or reflex movements. The
most common movement was finger jerks.
Undulating toe flexion sign, triple
flexion response, Lazarus sign,
pronation–extension reflex, and facial myokymia
also were seen.
These movements may be more common than reported
and do not preclude the diagnosis of BD.
______________________________________________________

J Korean Med Sci 2006; 21:
588-90
ISSN 1011-8934
Reflex Movements in
Patients with Brain Death: A Prospective Study
in A Tertiary Medical Center
Reflex movements have been reported to occur in
up to 75% of brain-dead patients,
but this issue has not been addressed in Korea.
The patients admitted to our hospital who met
the criteria for brain death were enrolled
between March 2003 and February 2005. The
frequency and type of reflex movements in these
patients were evaluated prospectively using a
standardized protocol. Brain death was
determined according to the guideline of Korean
Medical Association. Of 26 patients who were
included, five (19.2%) exhibited reflex
movements such as
the pronation
- extension reflex, abdominal reflex, flexion
reflex, the Lazarus sign, and periodic leg
movements. This finding suggests that
the frequency of spinal reflex movements is not
rare and the awareness of these movements may
prevent delays in brain-dead diagnosis and
misinterpretations .
  
|
