|
1.
Maternal brain death; brain dead pregnant women who were deliberately
kept alive until their babies were ripe enough to be delivered. The
mothers were sacrificed thereafter.
2.
Case records of brain dead patients who regained their consciousness
after being formally pronounced brain dead. The reports came from: USA, UK
and Saudi Arabia.
3.
The Lazarus sign (L.S.): spontaneous, complex purposeful movements of
the limbs and the trunk in the so called "brain dead"
patients who cough and try to breathe during apnea testing.
4.
Chronic brain death: some studies done by the American academy of
neurologists and others which prove that some brain dead patients
survived for periods exceeding 14 years.
------------------------------------------------------------------------------------------------------------------------------
1. Maternal brain death
As the year 1968 witnessed
the 1st world wide legal recognition
of brain death by the declaration of the Harvard criteria defining
it, the year 1982(1) witnessed the 1st
heavy blow received by the proponents of this concept. This blow was
a case report that appeared in the JAMA declaring the successful
attempt made by the authors to sustain (or prolong) the life of a
pregnant brain dead mother for a few weeks until she delivered a
healthy baby. This was described at that time as "the straw that
broke the camel's back". More research continued in the
years to come until in 1988(2) another report
appeared in JAMA emphasizing the capability of brain dead pregnant
women to give birth to healthy babies. Ever since then, many other
case reports have appeared in the literature that it became a well
recognized "fact" known under the heading of maternal brain
death. It is to be noted that a single study reported in the journal
of critical care medicine in 2003(3) involved 11
cases, 10 to whom continued their pregnancy and gave birth to normal
healthy babies. The next three films show three cases of brain dead
mothers that have been kept alive on advanced life support for
several weeks until their babies were mature enough to be delivered.
The mothers were sacrificed afterwards .

|

Crit Care Med. 2003 Apr; 31(4):1241-9.
Extended somatic support for pregnant women after brain
death.
Powner DJ, Bernstein
IM.
Department of Neurosurgery, University
of Texas, Houston, TX,
USA.
OBJECTIVE: To review case reports of pregnant women
who have been supported after brain death until successful delivery
of their infants. From these reports and other literature about
brain death, normal physiologic changes of pregnancy, and specific
needs for fetal development, recommendations were made to assist in
supporting pregnant women after brain death until delivery of a
mature fetus who is likely to survive.
DATA SOURCES: Personal files and experiences,
MEDLINE review of case reports and publications about physiologic
changes present during normal pregnancy and after brain death, and
the critical needs for fetal development were included. DATA
EXTRACTION: Eleven reports
of ten patients comprise the accumulated clinical experience.
Hypotension, requiring fluid administration and inotropic/vasopressor
therapy, occurred in all the mothers, and in six cases, was the
reason for urgent delivery. The
longest period of support was 107 days, from 15 to 32 wks of
gestation. Two mothers also became organ donors.
Recurrent infections, thermolability, and
other complications common to prolonged ICU care were encountered.
All infants survived. One had congenital abnormalities caused by phenytoin use by the mother. When followed, all
others developed within normal growth and mental variables. These
cases plus literature citations noted above were used to develop
recommendations for maternal/fetal care.
CONCLUSION: Preservation of uterine/placental blood flow is the
most important priority during somatic support. Imprecise autoregulation of the uterine vasculature
during maternal hypoxemia or hypotension makes this goal a
significant challenge. Special considerations for nutrition;
medication use; cardiovascular, respiratory, or endocrine therapy;
fetal monitoring; hormone replacement; and ethical concerns are
discussed.
|

Reprod Health. 2006 Apr 27; 3:3.
The prolongation of somatic support in a pregnant woman with
brain-death: a case report
Souza
JP, Oliveira-Neto A, Surita FG, Cecatti JG, Amaral E, Pinto
e Silva JL.
Intensive
Care Unit, Department of Obstetrics and Gynecology, School of Medical
Sciences, State University of Campinas,
Campinas, São Paulo, Brazil.
souzajpd@unicamp.br
BACKGROUND: Medical literature has increasingly
reported cases of maternal brain death during pregnancy. This is a
rare situation which demands the decision and, depending on the
gestational age, the implementation of a set of measures to prolong
the homeostasis of the human body after brain death for the purpose
of maintaining the foetus alive until its
viability. CASE PRESENTATION: A
40 year old woman suffered an intracranial haemorrhage during
the 25th week of pregnancy. Despite neurosurgical drainage
of a gross intraparenchymatous haematoma, the patient developed brain death.
Upon confirmation of this diagnosis, she received full ventilatory and nutritional support, vasoactive drugs, maintenance of normothermia, hormone replacement and other
supportive measures required to prolong gestation and improve the
survival prognosis of her foetus. All
decisions regarding the patient's treatment were taken in consensus
with her family. She also received corticosteroids to accelerate foetal lung maturity. During the twenty-five days
of somatic support, the woman's condition remained stable; however,
during the last seven days the foetus
developed oligohydramnios and
brain-sparring, which led the medical team to take the decision to
perform a Caesarean section at that moment. After delivery, the
patient's organs were removed for donation. The male infant was born
weighing 815 g, with an Apgar score of 9
and 10 at the first and fifth minutes, respectively. The infant was admitted to the neonatal
intensive care unit, but did not require mechanical
ventilation and had no major complications. He was discharged at 40 days of life, with
no sequelae and weighing 1850 g. CONCLUSION: These results
are in accordance with findings from previous studies and case
reports suggesting the appropriateness and safety of extended somatic
support during pregnancy under certain circumstances. They also
suggest the need for prompt diagnosis of brain death before the
occurrence of physiological degeneration, rapid evaluation of foetal status and the decision of the family
together with the medical team to prolong maternal somatic support.
The occurrence of maternal brain death is a tragedy, but it may also
represent a challenging opportunity to save the life of the foetus and, in addition, permit donation of the
maternal organs.

Obstet Gynecol Surv. 2000 Nov; 55(11):708-14
Irreversible
maternal brain injury during pregnancy: a case report and review of
the literature
Feldman
DM, Borgida AF, Rodis JF, Campbell
WA.
Department of
Obstetrics and Gynecology, University of Connecticut
Health Center,
Farmington 06030-2950, USA.
dfeldman@nso2.uchc.edu
Maternal
brain death or massive injury leading to persistent vegetative state
during pregnancy is a rare event. Since 1979, 11 cases, including the current one, of
irreversible maternal brain damage in pregnancy have been reported. In all but one, the pregnancies were prolonged
with a goal of achieving delivery of a viable infant.
Current advances in medicine and critical care enable today's
physician to offer prolonged life-support to maximize the chances for
survival in the neonate whose mother is technically brain dead. We
present a case at our institution and review all previously published
cases in the English literature for comparison as well as make
management recommendations.
Journal
of the American Medical Association

JAMA. 1988
Aug 12; 260(6):816-22.
Maternal brain death during pregnancy. Medical and ethical
issues.
Field DR, Gates EA, Creasy RK, Jonsen
AR, Laros RK Jr.
Department of
Obstetrics, Gynecology, University
of California, San Francisco
94143-0132.
We present in
detail a case of a 27-year-old primigravida
who was maintained in a
brain-dead state for nine weeks. An apparently normal and healthy male infant
weighing 1440 g was delivered. The
newborn did well and was found to be growing and developing normally
at 18 months of age. Although the technical aspects of
prolonged life support are demanding and the economic costs are very
high (+217,784), there are ample ethical arguments justifying the
separation of brain death and somatic death and the maintenance of
the brain-dead mother so that her unborn fetus can develop and
mature.
KIE:
Physicians and an ethicist at the University
of California, San Francisco,
present the details of the case of a pregnant, brain-dead woman whose
vital functions were maintained for nine weeks until the delivery of
a healthy infant at 31 weeks' gestation. Despite the technical
difficulties involved and the economic costs incurred ($183,031 for
maternal care and $34,703 for neonatal care), the authors conclude
that ethical considerations support the decision on care. They argue
that the woman was not injured; that nonmaleficence
and beneficence toward the fetus require a rescue attempt if there is
a reasonable chance of reaching fetal maturity; that maternal medical
care may be more cost effective than prolonged neonatal support; and
that the father's wishes were respected. Rather than proposing
guidelines, they hold that decisions on prolonged maternal support
should be based on the circumstances of each case.
Journal of the American Medical Association

JAMA. 1982
Sep 3; 248(9):1089-91
Life support and maternal death during pregnancy
Dillon WP,
Lee RV, Tronolone MJ, Buckwald
S, Foote RJ.
KIE: The authors
are physicians affiliated with the State University of New York at Buffalo and the Children's Hospital of Buffalo.
They describe the clinical management of two brain-dead pregnant women and suggest
guidelines to help physicians decide whether to treat such women.
Based on the dramatically increasing chances for fetal survival from
the 24th to the 27th weeks of gestation, they recommend vigorous life
support during this period to permit fetal viability and prognosis to
be assessed. Fetuses of 28 weeks
should be delivered by cesarean section as soon as practicable after
confirmation of maternal brain death.
|
Promoting thoughtful, balanced reflection
on the ethical and social issues of medicine and medical science
|
 
|
Hastings
Cent Rep. 1986 Feb; 16(1):12-7
On dying more than one deathShrader D
.
Death
(with a capital D) can best be understood as a series of distinct but
related deaths. For example, a pregnant woman was found to be brain-dead but
her vital functions were artificially sustained for nine weeks until
her fetus could be delivered, after which the machines were removed
and she died a second, conceptually distinct death.
This procedure is probably justifiable, but any legislation or policy
regarding such cases should be flexible and should require consent.
KIE:
It is argued that death should be understood as encompassing a series
of distinct but related events. Human beings are viewed as a
composite of two intimately related but distinguishable components,
as both persons and biological entities. Thus, a brain dead patient
can be considered in some sense alive and in some sense dead. This
thesis forms the basis for an analysis of a case in which a brain
dead pregnant woman's vital functions were artificially sustained
until her fetus could be delivered alive, after which the woman's
life support systems were disconnected and she ceased breathing. The
author holds that this procedure was morally justifiable. He suggests
that a multiple-deaths analysis may provide a general framework for
discussion of the conditions that justify maintenance of biological
functions in neocortically dead human
beings, but cautions that any legislation or policy regarding such
cases should be flexible and should require consent.
Revista médica
de Chile

Rev Med Chil.
1998 Apr; 126(4):450-5.
Maternal
brain death during pregnancy
[Article
in Spanish]
Beca JP, Wells W, Rubio W.
Facultad
de Medicina, Universidad de Chile.
The
case of a pregnant patient who had a massive intracraneal
haemorrhage at 18 weeks of gestation is
presented. Patient's neurological damage
evolved to brain death, but the fetus continued in good condition.
The decision of withdrawing life support or to continue supporting
the mother's life to allow fetal development aroused difficult
ethical questions, both to relatives and professionals. This is an
exceptional situation of a heart beating cadaver and a non viable
fetus whose life depends on the continuation of treatments that are
considered as experimental. A good decision should be based on the
respect to a body in brain death, the fetal right to life, family's
wishes and values, the use of experimental treatments, and the
rational use of a public hospital's resources. The conclusion was
that the continuation of life support treatments was not an ethical
obligation. Withdrawing life support to allow fetal death in this
case means foregoing an experimental treatment and to respect
family's autonomy and the right of the patient's death with dignity. Similar cases need to be
discussed with a multidisciplinary analysis in their own
particularity.

Critical
Care Clinics
Crit Care Clin.
2004 Oct;20(4):747-61
Cardiopulmonary
resuscitation and somatic support of the pregnant patient.
Mallampalli A, Powner DJ, Gardner
MO.
Section
of Pulmonary and Critical Care Medicine, Baylor College of Medicine,
Ben Taub General Hospital, 1504 Taub Loop, 6th Floor, Houston, TX 77030, USA.
antara@bcm.tmc.edu
Cardiopulmonary
arrest during pregnancy is a rare event that critical care clinicians
must be prepared to manage. The causes of cardiopulmonary arrest
during pregnancy, recommended modifications to cardiopulmonary
resuscitation protocols that are specific to pregnancy, indications
for and timing of perimortem cesarean
delivery, and the expected fetal outcomes are reviewed. Rarely, brain death of a pregnant patient may occur
in which continued support of the mother is possible to prolong the
pregnancy and improve fetal outcome. Prolonged somatic support
of pregnant patients who are brain dead presents specific management
challenges, but has been accomplished. The physiologic changes that
occur after brain death and recommendations for somatic support of
the brain dead pregnant patient also are reviewed.

Crit Care Med. 2005 Oct; 33(10 Suppl):S325-31.
Cardiac
arrest in pregnancy and somatic support after brain death.
Mallampalli A, Guy E.
Section
of Pulmonary and Critical Care Medicine, Department of Medicine,
Baylor College of Medicine, Houston, TX, USA.
OBJECTIVE:
To review the important causes of cardiopulmonary arrest during
pregnancy and the recommended modifications to resuscitation
protocols when applied to pregnant patients, including the
indications for perimortem cesarean section
and the expected fetal outcomes, and to review the literature
regarding extended somatic support after brain death during
pregnancy. DATA SOURCES: MEDLINE review of publications relating to
cardiac arrest and resuscitation in pregnancy, physiologic changes
after brain death, and attempted somatic support of brain-dead
pregnant women. CONCLUSIONS: Cardiac arrest during pregnancy is rare,
but it is important to recognize the causes, which may be either
unrelated to pregnancy or unique to the pregnant woman. For the most
part, the resuscitation protocol is the same as for nonpregnant victims of cardiac arrest, with a few
important modifications, including especially the need for relieving aortocaval compression by the gravid uterus, the
need for rapid intubation, and the importance of rapid perimortem cesarean delivery when indicated. In
those rare cases of brain death occurring in a pregnant patient,
continued somatic support of the mother may be possible, even for
prolonged periods, to extend the pregnancy and further fetal
maturation. The expected physiologic changes after brain death,
challenges to successful somatic support, and specific
recommendations regarding organ support of the brain-dead pregnant
woman are reviewed.
Neurocritical
Care
Neurocrit Care. 2005;3(2):99-106
Maternal
brain death and somatic support.
Farragher RA, Laffey
JG.
Department
of Anesthesia, University College Hospital, and Clinical Sciences
Institute, National University of Ireland, Galway, Ireland.
Brain
death is a concept used in situations in which life-support equipment
obscures the conventional cardiopulmonary criteria of death, and it
is legally recognized in most countries worldwide. Brain death during
pregnancy is an occasional and tragic occurrence. The mother and
fetus are two distinct organisms, and the death of the mother
mandates consideration of the well-being of the fetus. Where maternal
brain death occurs after the onset of fetal viability, the benefits
of prolonging the pregnancy to allow further fetal maturation must be
weighed against the risks of continued time in utero, and preparations must be
made to facilitate urgent cesarean section and fetal resuscitation at
short notice. Where the fetus is nonviable, one must consider whether
continuation of maternal organ supportive measures in an attempt to
attain fetal viability is appropriate, or whether it constitutes
futile care. Although the gestational age of the fetus is central to
resolving this issue, there is no clear upper physiological limit to
the prolongation of somatic function after brain death. Furthermore,
medical experience regarding prolonged somatic support is limited and
can be considered experimental therapy. This article explores these
issues by considering the concept of brain death and how it relates
to somatic death. The current limits of fetal viability are then
discussed. The complex ethical issues and the important variations in
the legal context worldwide are considered. Finally, the likelihood
of successfully sustaining maternal somatic function for prolonged
periods and the medical and obstetric issues that are likely to arise
are examined.
Journal
of transplant coordination

J Transpl Coord. 1997 Sep;7(3):103-5.
Dead
Organ recovery following childbirth by a brain-mother: a case report.
Lewis
DD, Vidovich RR.
Ohio Valley Life
Center, Cincinnati, USA.
Little
information is available in the medical and nursing literature
concerning organ recovery from brain-dead,
pregnant individuals. Many healthcare professionals might rule
out such patients as potential donors, especially if childbirth is a
possibility. This article presents an actual case study in which the birth of a healthy
infant and recovery of organs from the mother were successful. It also reviews the
available literature and discusses factors related to organ
placement.
Journal
of Obstetrics and Gynaecology

Obstet Gynecol.
1989 Sep;74(3 Pt 2):434-7.
Maternal
brain death and prolonged fetal survival.
Bernstein
IM, Watson M, Simmons GM, Catalano PM, Davis G, Collins R.
Department
of Obstetrics and Gynecology, Medical Center
Hospital, Vermont, Burlington.
A
30-year-old woman suffered massive brain injuries after a motor
vehicle accident at 15 weeks' gestation. The patient was diagnosed
as brain-dead on her tenth hospital day. She was supported with
intensive care for 107 days after this diagnosis
and a normal 1555-g male infant was delivered at approximately 32
weeks' gestation by repeat cesarean section. The child is developing
normally at 11 months of age. This represents the longest reported case of
prolongation of pregnancy after brain death
Minerva
Anestesiologica

A
Journal on Anesthesiology, Resuscitation, Analgesia and Intensive
Care
Minerva Anestesiol.
1992 Nov; 58(11):1247-52.
Brain
death and prolonged fetal survival
[Article in Italian]
Antonini
C, Alleva S, Campailla MT, Pelosi G, Valle E, Verrua M, Zamponi E,
Blanda A, Gambaro C.
Facoltà di
Medicina e Chirurgia,
Università degli Studi di Torino.
The
Authors presents in detail a case of a 25-year-old primigravida that had fatal intracranial bleeding
at the beginning
of the 15th week of gestation, whose vital function are sustained for
49 days. Despite the insuccess to bring the
pregnancy to a gestational period favorable to induce the delivery, they analyze the problems
connected to the maternal maintenance and to the fetal growth.
---------------------------------------------------------------------------------------------------------------------
2. Some documented
cases of the so called "brain death", who regained their
consciousness in the USA,
Britain and, Saudi Arabia
It
is to be noted that all cases mentioned in this text were formally
declared brain dead by a "three doctor committee" in
recognized centres and according to the
protocols adopted by these centres. The
families of these patients were asked for consent for organ donation
of their "deceased" ones. In some of these cases the
families agreed and preparations for organ harvesting were made while
in others the consent was denied and the families insisted on
continuing medical treatment. However all cases recovered (check the
details). It is worth mentioning that cases of brain death that
regain consciousness are deliberately ignored and hardly ever
referred to in public because of legal implications and liabilities.
The information usually leaks through the families to the media and
hence become recorded and published. This explains the reason for the
scarcity of the number of such cases that get exposed in public in
spite of being so plenty. This fact has recently been emphasized by
an Egyptian urosugeon (Dr. Hossam El-Din Mostafa,
ex-president of the Canadian society of urosurgeons,
Ontario, Canada,
and fellow of royal college of surgeons in London) in El-Ahram
newspaper on 9/2/2008. Dr. Hossam mentioned
a personal story that took place when he was an assistant of a
leading surgeon in one of the leading industrial countries. After the
kidneys had been harvested in a brain dead patient and at the end of
the procedure, the patient showed signs of life. The surgeon asked
Dr. Hossam to keep the secret to himself as
the patient's family might press charges (refer to the article).
Even
though transplant surgeons are always in a hurry to harvest organs
from patients as soon as they are declared brain dead (after six
hours and up to 24 hours at most according to the protocol used) and
by so doing they hardly give such patients any real chance to
recover. And inspite of the fact that
transplant surgeons are so discrete and are always so strict in
addressing the media trying to hide information concerning those
cases that recover after being diagnosed brain dead. Inspite of all that some information concerning
such cases manages to find its way to the media or to scientific
journals. And we are disclosing here in some of the documented cases
that have been officially declared or pronounced brain dead and yet
recovered and were hence published whether in scientific journals or
in the different media.
Case
1
 Friday February 15, 2008 Friday February 15, 2008
Woman
Diagnosed as "Brain Dead" Walks and Talks after
Awakening By
Hilary White
LAKE ELMO, Minnesota, February 15, 2008 (LifeSiteNews.com) -
65-year-old Raleane "Rae" Kupferschmidt's relatives were told by doctors
that she was "brain dead" after she had suffered a massive
cerebral haemorrhage in mid-January,
according to an Associated Press Report. Her family had taken her
home to die and was in the process of grieving and planning her
funeral when she awoke and was rushed back to hospital. In
accordance with her own wishes, doctors had
removed Rae's breathing tube and were waiting for her to die. She was
taken home from the hospital, and while friends and family gathered
to say a last good bye, Kupferschmidt's
daughter Lisa Sturm used an ice cube to wet her mother's dry lips.
When her mother sucked on the ice cube, she thought it was only an
instinctive reaction. She said, "I knew suckling is a very basic
brain stem function, so I didn't get real excited. But when I did it
again she just about sucked the ice cube out of my hand, and I looked
at my aunt and said, 'Did you see that?'" "So I leaned down
and asked, 'Mom... Mom, are you in there?'" Sturm said.
"And when she shook her head and mouthed, 'Yes,' we all just
about fell over." Rae was rushed back to the hospital and
underwent surgery to drain the blood clot from her skull. After surgery,
she recovered her strength and is now undergoing physical therapy and
can walk with the aid of a walker. Doctors expect her to be walking
on her own within weeks. Rae says she does not remember anything
during her coma. "I still don't know what my task is here on
this Earth, but I know God's not done with me yet. How else could you
explain everything that has happened to me?" Rae said. She told
family that she had seen angels in her room. "I said these
angels are not here to take me home to my father. They're here to
help me, to help me get over this. "Brain death" or
"death by neurological criteria," is common
media terminology for patients who are said to be in an
irreversible coma, sometimes referred to as a "persistent
vegetative state" (PVS) Physicians and bioethicists
who support "brain death" criteria claim that such a
diagnosis is reliable and means that a patient is beyond any hope of
recovery. Under new bioethics criteria, "brain death"
can be used as a condition under which organs are removed from a
patient while his heart is kept beating. Organ transplant requires
that tissue be recovered from donors as close to physical death as
possible and physicians are under heavy pressure to procure more
organs. The fact that in some cases patients who have been
unconscious, semi-conscious or severely neurologically disabled have
been declared "brain dead" or "PVS" only to
recover has undermined public confidence in the medical system. In
the US
in 2006, Terry Wallis, who experienced a car wreck in 1984, woke
unexpectedly and began to recover after 19 years in a minimally
conscious state. In 2005 in Italy, Salvatore Crisafulli woke from a coma he had suffered for
two years. He had been declared "nearly dead" by doctors
after a serious auto accident that left him unresponsive. In Poland
in 2007, a railway worker astonished his family and doctors when he
awoke spontaneously after 19 years. Doctors at United Hospital
said they are amazed by Rae Kupferschmidt's
recovery. One told Good Morning America, "I've been here for ten
years and I've never seen anything quite like this."
Rae told Good Morning America, "God's got something for me to
do. When I learn it, I'll unfold it and follow it."
Case 2

Mon March 24, 2008
Man
declared dead, says he feels 'pretty good'

This
photo provided by the NBC Today television program shows Doug Dunlap,
left, and his son Zach Dunlap, during their interview with Today show
correspondent Natalie Morales.24.3.2008
Story
Highlights
Family
members were paying last respects when Dunlap moved hand and foot
He
remembers hearing doctors pronounce him dead
Father
says brain scan showed no activity
Mother
says it was a miraculous feeling to discover son still alive
OKLAHOMA
CITY, Oklahoma (AP) -- Zach Dunlap says he
feels "pretty good," four months after he was declared
brain dead and doctors were about to remove his organs for
transplant.
Zach
Dunlap, 21, said he has no recollection of his crash.
 Dunlap was pronounced dead November 19 at United Regional
Healthcare System in Wichita Falls, Texas, after he was injured in an
all-terrain vehicle accident. His family approved having his organs
harvested. Dunlap was pronounced dead November 19 at United Regional
Healthcare System in Wichita Falls, Texas, after he was injured in an
all-terrain vehicle accident. His family approved having his organs
harvested.
As
family members were paying their last respects, he moved his foot and
hand. He reacted to a pocketknife scraped across his foot and to
pressure applied under a fingernail. After 48 days in the hospital,
he was allowed to return home, where he continues to work on his
recovery.
On
Monday, he and his family were in New York, appearing on NBC's
"Today."
"I
feel pretty good. but it's just hard ...
just ain't got the patience," Dunlap
told NBC.
Dunlap,
21, of Frederick,
Oklahoma, said he has
no recollection of the crash.
"I
remember a little bit that was about an hour before the accident
happened. But then about six hours before that, I remember," he
said.
Dunlap
said one thing he does remember is hearing the doctors pronounce him
dead.
"I'm
glad I couldn't get up and do what I wanted to do," he said.
Asked if
he would have wanted to get up and shake them and say he's alive,
Dunlap responded: "Probably would have been a broken window that
went out."
His
father, Doug, said he saw the results of the brain scan.
"There
was no activity at all, no blood flow at all."
Zach's
mother, Pam, said that when she discovered he was still alive,
"That was the most miraculous feeling."
"We
had gone, like I said, from the lowest possible emotion that a parent
could feel to the top of the mountains again," she said.
She said
her son is doing "amazingly well," but still has problems
with his memory as his brain heals from the traumatic injury.
"It
may take a year or more ... before he completely recovers," she
said. "But that's OK. It doesn't matter how long it takes. We're
just all so thankful and blessed that we have him here."
Dunlap
now has the pocketknife that was scraped across his foot, causing the
first reaction.
"Just
makes me thankful, makes me thankful that they didn't give up,"
he said. "Only the good die young, so I didn't go."
Case 3
The
Middle East's Leading English
Language Daily Monday 5 November 2007 (25 Shawwal 1428)
Woman
Declared Brain Dead Now Starts to Speak
Muhammad Al-Homaid, Arab News
YANBU, 5 November 2007 — The Yanbu General Hospital yesterday announced a
change in the condition of Fatima Rifaie, a
33-year-old Saudi woman who was declared brain dead following a
medical error three months ago.
“My sister’s condition has improved
considerably. She has begun recognizing and talking to relatives who
come to visit her,” Eid Rifaie, Fatima's
brother, told Arab News yesterday. However, Eid
added that it would take months before his sister returned to
normalcy.
Fatima,
who was a chronic asthma patient, went into a coma after she was
allegedly administered a banned antibiotic on Aug. 3. The doctor who
administered the injection, allegedly a Syrian, has been suspended.
Dr. Yaser Redwan, a heart consultant at Erfan
and Saiedi General Hospital in Yanbu, later examined Fatima
and said she was brain dead and that her heart had stopped as a
result of the injection. He said that the delay in
treating her after her condition worsened had resulted in brain
atrophy that later left her brain dead. Redwan
blamed the doctor for Fatima's
condition and said he had not tested to see whether the patient was
allergic to the antibiotic.
Fatima
was later transferred to King
Fahd Hospital
in Madinah. On Aug. 27, doctors reported
that she was not brain dead but that she was in a coma. After an
emergency surgery to revive her in Madinah,
she was sent back to the Yanbu hospital to
continue treatment.
Case
4
Asharq Alawsat
Newspaper
19/03/2006
LOS ANGELES (Reuters) -Doctors pronounced
Ethan Myers brain dead after a car accident dealt the 9-year-old a
severe brain injury in 2002. After he miraculously awoke from a
nearly month-long coma, doctors declared he would never again eat on
his own, walk or talk.
Yet, thanks partly to a video game system,
Myers has caught up with his peers in school and even read a speech
to a large group of students.
"I'm
doing the exact same things as them. I'm getting buddies and
stuff," said Myers, who had relearned to walk and was reading at
a second-grade level before his video game therapy began in May 2004.
"I
couldn't remember where I put stuff and now I can. I remember school
stuff and people's names," he said in a telephone interview from
his family's home in Colorado.
More
fundamentally, Myers can now fully open his right hand, which
paralysis had curled closed. His brother and sister, who were in the
car with him during the accident and each suffered mild brain
injuries, have also shown improvement in their memory and other
functions.
Ethan
and his parents attribute his most recent progress to neuro-feedback training on the Cyber Learning
Technology LLC system, which is often used to play car racing video
games. "In the last year, we've seen the Ethan we knew before
the accident," said Howard Myers, the teenager's father.
Case
5

DYING
TO LIVE Defining
death
Question
of brain death can complicate the ethics of organ donation
Monday,
November 15, 2004 by
DAVE PARKS
News
staff writer
The Florida
woman was pronounced brain dead at UAB Hospital
after suffering severe bleeding inside her head. Her family gave
doctors permission to remove vital organs for transplant. It
was around midnight, and surgeries — for the donor and recipients —
were scheduled the next morning, Sunday, Oct. 31. Meanwhile, the
donor's body was kept on a ventilator and given drugs to maintain
blood flow, all steps necessary to maintain organs for transplant.
Then everybody waited. But the unexpected occurred. During the night,
somebody in the intensive care unit saw the ventilator's light pop
on, an indication the woman was breathing on her own and wasn't brain
dead. An electroencephalogram,
or EEG, picked up what appeared to be electric signals in her brain. The organ procurement was canceled,
and everybody waited some more. Dr. Steve Bynon,
a transplant surgeon at the University
of Alabama at Birmingham,
said the incident was unusual, but it showed that medical safeguards
work. Organs are not taken from donors whose brains are still alive.
"We just aren't an organ mill."
Case
6

Christina
after the announcement of the pretended diagnosis of brain death

Christina
after the awakening
news.webshots.com
On July 15,
2004, Christina Nichole went into a coma following one-time
hypoglycemic episode. All of her organs went into failure and they
told us that her brain was gravely deprived of oxygen. She was put on
full life-support and declared globally brain damaged and brain dead
except for a tiny spotty portion of the bottom of her brain stem. She
developed Adult Respiratory Distress Syndrome (ARDS), pneumonia,
blood sepsis, Staph, and other
life-threatening infections. Her prognosis was "NIL chance of
recovery". On the sixth day her father and I were asked to allow
them to turn off her life support machines. By this time she had
somehow overcome the organ failures, ARDS, pneumonia, sepsis, and
infections so we also had to consider organ donation from our 32 year
old daughter's body. Her doctors told us that if we did not allow her
to be 'let go' (killed from reduction/withdrawal of life support
care) we would destine her to live the rest of her life in a
persistent vegetative state with no 'quality of life'. Christina had
responded to me for the first time that same morning by blinking her
eyes ever so slightly on my command, so we did not believe their
objective tests. We requested absolute proof of their diagnosis and
prognosis with testing that we felt was the minimum of routine
procedures in cases like this, an EEG, CAT scan, and MRI. Our
requests were flatly denied on the grounds that no further testing
was warranted because her doctors 'already knew' what the tests would
show them; that she was 'gone' and would never come back. They were wrong! We learned two years later
that they had actually performed a CAT scan that showed NORMAL results. Why did they refuse to tell us
about the test and why did they continue to insist that we sign the euthanization papers, always telling us she was
already dead? They LIED to us, over and over again, in masse. They
were angry with us but we stood our ground... praise God! Judy
Case 7
Is
a miracle to Life
teen who was once 'brain dead'
Deseret News (Salt Lake City), May 21, 2005 by Sara Israelsen Deseret
Morning News
PROVO
-- When Derek Maughan goes to get a
burger, it's a big deal. Cruising to a local fast-food place may
not seem like much to other 17-year-olds, but for this survivor it
seems like a miracle. When he was 2 months old, Derek's skull was
shattered in a car accident. Doctors declared him to be brain dead.
However, the little boy's parent's didn't buy the initial
prognosis, and 50 brain operations later, Derek is now a happy,
healthy teen who just got his driver's license. Shortly after the
accident and a helicopter ambulance trip to Primary Children's Medical Center,
little Derek fell into a coma. While in the coma he developed a
condition in which his blood wouldn't clot. He was still on the
blood clotting medication when he came out of the coma only to
develop a few weeks later a condition called hydrocephalus, a
swelling of the brain caused by excess fluid. Doctors inserted a shunt
to drain the fluids and he was finally able to go home. Soon, he
was spending countless hours with therapists, neurosurgeons and neurologists. A new scare came on
Derek's first birthday, when he began vomiting uncontrollably. His
mother, Jan'a, rushed him to the
hospital. An infection had developed in the shunt, and as a result
the boy was scheduled for the first of a long series of surgeries.
It's been a bumpy road, but Jan'a Maughan says it has been a road filled with
miracles.
Case
8
Rail
crash victim's `miracle' recovery
Independent on Sunday, the, Mar 21, 2004 by Stephen Seawright in
Hong Kong
A Hong Kong
television journalist who was declared brain- dead after being
critically injured in the Potter's bar train crash has made a
miraculous recovery and is finally hoping to return to work. Two of Tanya Liu's friends
died in the crash in May 2002. Ms Liu has spent the past two years in
rehabilitation in a hospital in Beijing.
She spent two months in a coma after the crash and was not able to
stand up unaided until near the end of 2002. In the year after the
crash, Ms Liu was operated on six times - twice for brain surgery. Ms Liu's family claim that British doctors declared her brain dead
shortly after the crash. But the family sought a
second opinion from a Beijing
neurosurgeon, who flew to London and said she could recover.
A month after the crash, Ms Liu's family transferred her to a hospital
in the Chinese capital and in July 2002 she came out of the coma. Seven people died when the
last carriage of the train traveling from King's Cross to King's Lynn derailed at Potters Bar station. Ms Liu's family claim that
in the first few weeks after the crash, doctors at the Royal Free
Hospital in north London urged
them to allow her to die. A
spokesperson for the Royal Free said: "I can't comment on
conversations between individuals, but some of these are not the kind
of expressions doctors use in these situations. Brain injury is a
highly complex area of medicine and one in which it is very difficult
to predict the degree and course of any patient's recovery. Ms Liu
suffered a very severe injury and we were very worried about her
future prospects."
Case
9
Anesthesiology:
Volume 91(1) July 1999 pp 275-287
A
Matter of Life and Death: What Every Anesthesiologist Should Know
about the Medical, Legal, and Ethical Aspects of Declaring Brain
Death
Van Norman, Gail A. MD
Case
3: An anesthesiologist requests that his/her department review the
events surrounding a potential organ collection. A young woman
receiving intravenous magnesium sulfate for pregnancy-induced
hypertension suffered seizures several hours after vaginal delivery.
After the seizures, she was unarousable and
posturing. She was intubated after
intravenous administration of 4 mg pancuronium,
and a computed tomography scan showed coning, diffuse edema, and
occipital lobe infarcts. A neurologist determined that the patient
had suffered a "catastrophic neurologic
event." Intravenous esmolol that was
being infused to control blood pressure and heart rate was
discontinued, and permission was obtained from the patient's family
for the patient to become a vital organ donor. On the day of
anticipated organ collection, the anesthesiologist found that the
donor had small, reactive pupils, weak corneal reflexes, and a weak
gag reflex. The esmolol infusion was
reinstituted. Further review of the patient's chart showed the
previous administration of pancuronium, and
a serum magnesium level of 5.1 mEq/l,
more than 2.5 times normal several hours after the magnesium infusion
had been discontinued. After
the anesthesiologist administered edrophonium
10 mg intravenously, the patient coughed, grimaced, and moved all
extremities. Vital organ collection
was canceled, and after consultation with a neurosurgeon, the patient
underwent placement of an intracranial pressure monitor. Intracranial
pressure was initially 18 cm H2O and gradually decreased
with therapy to 10 cm H2O. The patient ultimately regained
consciousness and was discharged home. She was alert and oriented but suffered from
significant neurologic deficits.
Case
10
Case 11
"Surprise for doctors
- organ donor still alive"
Orlando
Sentinel, 9/29/90.
Curt Coleman Clark
Doctors were about to
remove the organs of a 22-year-old North Carolina man they thought
had been killed in a traffic accident when his foot twitched. Curt was pronounced
"brain dead" and his family agreed to donate his organs.
But, after his foot moved, he was taken to the intensive care unit of
Baptist Hospital in Winston Salem where more signs of life were
detected
Case 12
(USA Today, Feb. 14,
1989).
Another
amazing case involving the recovery of one who was “brain dead”
happened in December 1988. Barbara Blodgett, a 24-year-old Washington state
woman who had been in a deep coma for more than five months, gave
birth to a healthy baby boy and then came out of the coma and began
making gradual progress toward recovery.
When thirteen-weeks pregnant on June 30, 1988, Barbara was severely
injured when the car she was riding in was struck by a drunk driver.
Her cousin was killed in the crash and she suffered head injuries so
severe that doctors proclaimed
she was in a state of “cerebral death.” Yet by January 1989 she was
asking questions, forming words, recognizing her family and friends,
and helping in small ways to care for her newborn baby.
Barbara spelled out the following message by pointing to letters on a
piece of paper: “Never give up”
Case no. 13-15 in Britain
October, 1980
On October 13th,
1980 a documentary film was broadcasted in the BBC concerning brain
stem death (BSD) under the heading:
Are
the donors really dead?
This film caused a sort of
unrest in the British society and lead to a recession of the public
support for organ donation due to the facts that it enclosed.
Proponents of organ transplantation exerted a big deal of effort to
overcome the serious repercussions of broadcasting this film. This
film shed the light on the concept of BSD as well as on the
controversies concerning the adoption of this concept versus the
concept of whole brain death which gained wide support in the USA.
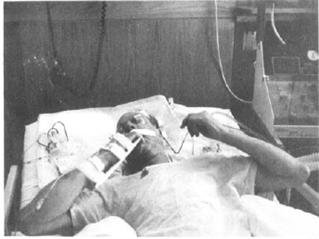
3. The
Lazarus phenomenon
Patients suffering from the
so called "Brain Death" can move their trunks and
extremities (spontaneous, complex and purposeful movements) as if
struggling to breathe after turning off the ventilator.
References of organ
transplantation frankly admit that the most serious obstacle that
faced the "lie of brain death" ever since it evolved was
the frequently recurring spontaneous movements in patients formally
diagnosed brain dead and awaiting organ harvesting. These movements
extend to involve the fingers, hands, arms and shoulders as well as
the feet and toes together with movements of the trunk (patients
trying to rise up and struggle to breathe) along with dozens of other
different forms of movements. And since these movements keep
recurring in such patients it couldn't be ignored or overlooked and
hence was termed "The Lazarus phenomenon".
"Lazarus" is the name of the man that had been raised from
the dead by Master Jesus as the bible states. For this reason the
term "Lazarus" is given to the brain dead patient who
experiences such movements along with other signs of life.
The
"Lazarus sign" startles equally, both families and
doctors:-
Some references describe
"Lazarus phenomenon" as most startling for both families
and doctors when they are faced by a moving "corpse" that
exhibits spontaneous, purposeful complex movements, who tries to get
up and struggles to breathe. Transplant doctors deny his being alive
and bounce on him to extract his organs.
The incidence of this
phenomenon amounts to 70-75% of cases.
This phenomenon is most
obvious at the time when the ventilator is turned off during what's
known as the "apnea test".
The muscular activity
exhibited in the "Lazarus phenomenon" may take different
forms like for instance grasping hands together, moving the legs as
if walking, moving hands to shoulders or below chin or intentionally
closing arms and this is why they are described as "complex and
purposeful" movements.
The "Lazarus
sign" is not confined to the moment when hypoxemia occurs as a
result of turning the ventilator off during apnea testing. It may
take place spontaneously or as a result of pain or any other sensory
stimuli.
The episode of muscular
activity may last a few minutes [exceeding 3.5 minutes in some cases
that were video taped]
Not only does the
"Lazarus sign" comprise moving the head or extremities and
shoulders but it may extend to involve other signs of life such as:-
1. Coughing.
2. Rhythmic shallow irregular respiratory activity
that may last for sometime after turning off the ventilator.
3. Moving the head sideways.
4. Repeated tremors of fingers and spastic
movements of lower jaw and face that may last for a few seconds.
The documents that prove
the fallacy of the claims denoting that "Lazarus sign" is
nothing but a reflex action arising in the spinal cord.
Recent articles that
are enclosed in the following pages prove that the type of movements
encountered in "Lazarus sign" go far beyond what was first
thought and that they are difficult to classify. Besides, most of
these movements follow a sequential pattern as if to achieve a
certain purpose. For this reason it becomes obvious that it is no
longer acceptable for transplantation proponents to assume that such
movements are nothing but spinal reflexes.
A study done in 2005 by the
American college of neurologists in New York admitted frankly that the
nature of the pathophysiology of L S
remained speculative. The study also suggested a new term for this
intriguing phenomenon: "brain death associated automatism".
This confession actually denounces all the claims put forth by
transplantation proponents trying to explain "Lazarus sign"
in brain dead subjects. This confession also denotes the fall of the
concept of brain death altogether as it is absurd to encounter
automatism in a "dead body".
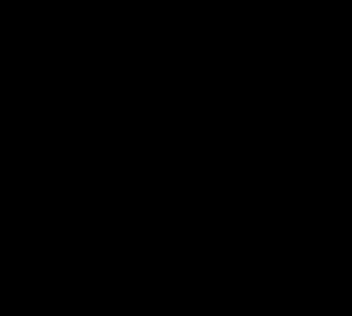
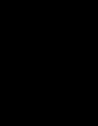
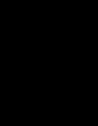
A: the body in a state of relaxation
B: the left elbow is rotated and the arm moves
closer to the body
D: both arms move when the left shoulder is
pinched
Source:
NEUROLOGY 2000; 54:224–227
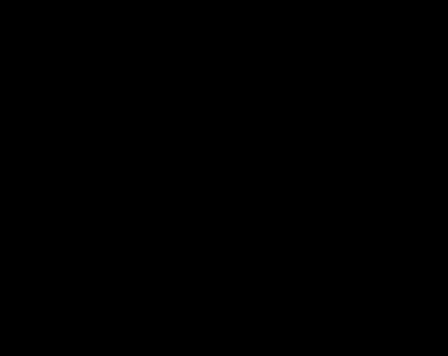
Brain
dead infant 11 months old
A: the body in a state of relaxation
C: the left elbow is medially closer to the body
The
same child grips the doctor's hand firmly and the doctor can hardly
loosens the child's grip to take away his hand
Source: NEUROLOGY 2000; 54:224–227
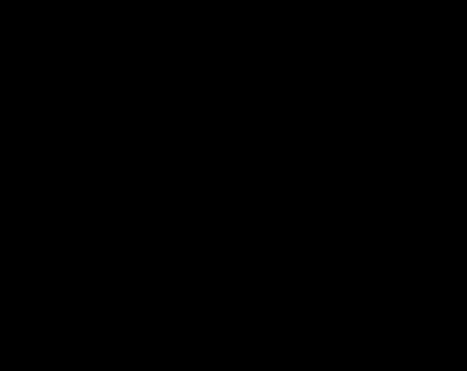
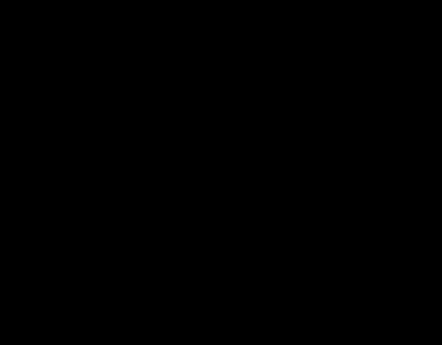
Source:
NEUROLOGY 1984; 34:1089
Lazarus
sign in a 43 year old Japanese patient during apnea testing
Department
of Anesthesiology & Critical Care Medicine,
Ajou University
Hospital
Medical
references for the Lazarus sign
Neurocritical
care
Neurocrit
Care.2005,3(2):122-6
Brain
death-associated reflexes and automatisms
Samay Jain1 and
Michael DeGeorgia2
Abstract
Background: In several instances, the diagnosis of brain death has been
questioned due to the presence of movements. This case report and review
of the literature illustrates the spectrum of movements that have
been encountered in brain death.
Methods:
A case report and review of the literature on movements seen in brain
death was conducted.
Results: Movements
in brain death are common and have a wide range of phenomenology.
Several movements wax and wane over time, making movements in brain
death difficult to classify. In
addition, varying terminology has been used (e.g., Lazarus sign,
spinal man, spinal reflexes, and spinal automatisms). Although
evidence points to a spinal origin for such movements, the pathophysiology in many cases remains
speculative. Characteristics of movements in brain death have been
identified that can help differentiate them from brainstem or
voluntary origin.
Conclusions:
Based on our review, we suggest referring to stimulus-provoked
movements as reflexes and spontaneous movements as automatisms. We propose using the
terms brain death-associated reflexes and brain death-associated
automatisms as two main
categories for movements that occur in brain death. These terms do not imply a specific pathophysiology,
but consistent clinically oriented nomenclature may be useful when
reporting such phenomena.
European
Journal of Neurology

Eur J Neurol.
2004 Nov; 11(11):723-7.
Undulating
toe movements in brain death
Saposnik G, Mauriño J, Saizar R, Bueri JA.
Movements in Brain Death Study Group,
Department of Neurology, Hospital JM Ramos Mejía,
Universidad de Buenos Aires, Buenos Aires, Argentina.
gsaposnik@yahoo.com
For many years, death implied immobility.
Nevertheless, there are anecdotal reports of spontaneous or reflex
movements (SRMs) in patients with Brain
death (BD). The presence of some movements can preclude the diagnosis
of BD, and consequently, the possibility of organ donation for
transplantation. McNair and Meador
[(1992), Mov Dord7: 345-347] described the
presence of undulating toe flexion movements (UTF) in BD patients.
UTF consists in a sequential brief plantar flexion of the toes. Our
aim was to determine the frequency, characteristics and predisposing
factors of UTF movements in a prospective multicenter
cohort study of patients with BD. Patients with confirmed diagnosis
of BD were assessed to evaluate the presence of UTF using a
standardized protocol. All patients had a routine laboratory
evaluation, CT scan of the head, and EEG. Demographic, clinical, hemodynamic and blood gas concentration factors
were analyzed. Amongst 107 BD patients who fulfilled the AAN
requirements, 47 patients (44%) had abnormal movements. UTF was
observed in 25 (23%) being the most common movement (53%). Early
evaluation (OR 4.3, CI95% 1.5-11.9) was a predictor of UTF in a
multivariate regression model. The somato-sensory
evoked potential (SSEPs) as well as
brainstem auditory evoked potentials (BAEPs)
did not elicit a cortical response in studied patients with UTF. This
spinal reflex is probably integrated in the L5 and S1 segments of the
spinal cord. Abnormal movements are common in BD, being present in
more than 40% of individuals. UTF was the most common spinal reflex.
In our sample, early evaluation was a predictor of UTF. Health care
professionals, especially those involved in organ procurement for
transplantation, must be aware of this sign. The presence of this
motor phenomenon does not preclude the diagnosis of BD.
Transplantation
Proceedings
Transplant
Proc.2004 Jan-Feb, 36(1):17-9
Frequency
of spinal reflex movements in brain-dead patients
Authors:
Dosemeci L.1; Cengiz M.; Yilmaz
M.; Ramazanoglu A.
Spontaneous and reflex movements may occur
in brain-dead patients. These movements originate
from spinal cord neurons and do not preclude a brain-death diagnosis.
In this study, we sought to determine the frequency and characteristics of
motor movements in patients who fulfilled diagnostic criteria for
brain death. Patients admitted to our department between
January 2000 and March 2003 and diagnosed as brain-dead were
prospectively evaluated in terms of spinal reflexes. Clinical brain
death was diagnosed according to our national law. We also prefer to
document the diagnosis of brain death with an EEG and/or TCD. Spinal
reflex movements were observed in 18 out of 134 (13.4%) brain-dead
patients during the study period. Lazarus sign, the most dramatic and complex
movement seen in brain-dead patients, was observed a few times
in two patients during an apnea test, an oculocephalic
test, after a painful stimulus, and after removal of a ventilator.
The other reflex movements observed in our brain-dead patients were
finger and toe jerks, extension at arms and shoulders, and flexion of
arms and feet. The occurrence of spinal reflexes in brain-dead
patients may certainly delay decision making, such as starting a
transplantation procedure, because of difficulties in convincing the
family or even a physician taking part in the diagnosis of brain
death. An
awareness of spinal reflexes may prevent delays in and
misinterpretations of the brain-death diagnosis
Acta Neurol
Scand. 2003 Sep, 108(3):170-3
Complex
spinal reflexes during transcranial Doppler
ultrasound examination for the confirmation of brain death
Authors: de Freitas, G. R.1; Lima, M. A. S.
D.1; André, C.1
Abstract:
De
Freitas GR, Lima MASD, André C. Complex spinal reflexes during
transcranial Doppler ultrasound examination for the confirmation of
brain death.
Acta Neurol
Scand 2003: 108: 170-173. © Blackwell Munksgaard
2003. Objective
Complex
sets of movements of the extremities can be seen in patients with
brain death (BD), and are typically observed during apnea testing or
removal of ventilatory support (also called
the Lazarus sign). We here describe brain-dead patients who had not
shown previous movements, even during apnea testing, but presented
complex spinal reflexes during transcranial
Doppler (TCD) examination elicited by neck flexion. Methods -
We
performed a prospective TCD study of patients with the clinical
diagnosis of BD. Results
Four
(2.5%) of 161
brain-dead patients presented complex spinal reflexes exclusively
during TCD examination.
TCD showed vertebro-basilar circulatory
arrest in all four. Their systolic blood pressure was significantly
lower than that of brain-dead patients not presenting movements during
TCD examination.
Conclusions: Hypotension and mechanical stimulation play a
role in the pathophysiology of complex
spinal reflexes present in BD, which are not exclusively seen in
terminal hypoxia. Intensive care personnel and neurologists who
perform TCD to confirm BD should be aware of these movements.
Journal
of the American
Academy of
Neurology
Neurology 2000, 54:221
Spontaneous
Movements Often Occur After Brain Death
Science Daily — ST. PAUL, MN - Many brain-dead patients have
spontaneous movements such as jerking of fingers or bending of toes
that can be disturbing to family members and health care
professionals and even cause them to question the brain-death
diagnosis. These
movements occur in 39 percent of brain-dead patients, according to a
study published in the January 11 issue of Neurology, the scientific
journal of the American
Academy of
Neurology.
"We found that these movements are more
common than has been reported or believed,"
said neurologist and study author José Bueri,
MD, of J. M. Ramos
Mejia Hospital
in Buenos Aires, Argentina. "People
need to know that these movements are spinal reflexes that do not
involve any brain activity."
The
study examined all patients at the hospital during an 18-month period
with a diagnosis of brain death. Of the 38 patients, 15 had these
motor movements. In all cases, the movements were seen in the first
24 hours after brain death diagnosis, and no movements were seen
after 72 hours.
Some
of the movements occurred spontaneously; others were triggered by
touch. Examiners used tests designed to elicit motor movements, such as
lifting the arms or legs or touching the palm of the hand.
Electroencephalogram
(EEG) tests did not show any brain activity in any of the patients
with movements.
"If
the lack of understanding of these movements leads to a delay in the
brain death diagnosis or questions about the diagnosis afterwards,
there can be important practical and legal implications, especially
for organ procurement for transplantation," Bueri
said. "Family members and others need to understand that these
movements originate in the spinal cord, not in the brain, and their
presence does not mean that there is brain activity.
One of the most startling movements for
family members and health care professionals is called the 'Lazarus
sign.' It is a sequence of movements lasting for a few seconds that
can occur in some brain dead patients, either spontaneously or right
after the ventilator is disconnected," Bueri
said. It is named for the episode in the Bible where Lazarus is
raised from the dead.
"It starts with stretching of the arms,
followed by crossing or touching of the arms on the chest, and
finally falling of the arms alongside the torso," he said.
"It is also a spinal reflex, but it can be disturbing to family
members and others who see this."
Another
article in this issue of Neurology describes unusual movements in two
brain dead patients. The movements occurred in a 30-year-old woman
and an 11-month-old
baby at a hospital in Barcelona,
Spain.
Both patients extended their arms, flexed their wrists and curled up
their fingers each time the mechanical ventilator inflated their
lungs. The movements stopped after the patients were disconnected
from the ventilator.
"We had never seen these type of
movements before, and they hadn't been reported in the medical
journals," said neurologist Joan Martí-Fàbregas,
MD, PhD, of the Hospital de la Santa Creu i Sant Pau.
The
doctors conducted additional tests and confirmed that there was no
brain activity. "The living cells that were ordering these
muscles to move were not brain cells or brain stem cells, but cells
located in the spinal cord," he said. "It's important for
family members and health care professionals to be aware of this
possibility."
A
neurologist is a medical doctor with specialized training in
diagnosing, treating and managing disorders of the brain and nervous
system.
The American Academy
of Neurology, an association of more than 16,000 neurologists and
neuroscience professionals, is dedicated to improving patient care
through education and research.
The American Journal of
Medicine
Volume
118, Issue 3, March 2005, Pages 311-314
Spontaneous
and reflex movements in brain death
G. Saposnik, MD, J. A. Bueri,
MD, J. Mauriño, MD, R. Saizar,
MD and N. S. Garretto, MD
From
the Department of Neurology, Hospital J.M. Ramos Mejía,
Buenos Aires, Argentina.
Address
correspondence and reprint requests to Dr. José A. Bueri, Department of Neurology, Hospital J.M.
Ramos Mejía, Urquiza
609, Buenos Aires (1221), Argentina.
Spontaneous and reflex movements may be
found in patients with brain death (BD). The authors
prospectively evaluated their frequency using a
standardized protocol. Among 38 patients who fulfilled criteria
for BD, the authors found 15 (39%) with spontaneous or
reflex movements. The most common movement was finger jerks. Undulating
toe flexion sign, triple flexion response, Lazarus sign, pronation–extension reflex, and facial myokymia also were seen.
These movements may be more common than reported and
do not preclude the diagnosis of BD.

J
Korean Med Sci 2006; 21: 588-90
ISSN
1011-8934
Reflex
Movements in Patients with Brain Death: A Prospective Study in a Tertiary Medical Center
4. Chronic
"brain death"
Some
studies done by the American academy of neurologists and others which
prove that some brain dead patients survived for periods exceeding 14
years simply because they were properly looked after.
In
order to fool public opinion, transplantation proponents continuously
claimed that deeply comatose patients whom they presume to be brain
dead cannot survive beyond two weeks no matter what. As a matter of
fact this assumption contradicts medical documents as is clear from
the following:-
1. From the research conducted by the American
academy of neurologists concerning the life expectancy of brain dead
patients it was found that many of such patients can survive from one
to 14 years simply if they are properly cared for.
2. Such patients are referred to as "chronic
brain dead". Chronic brain death refers to a state in which the
heart of patient, even after being pronounced brain dead, does not
stop beating for an extended period of time.
3. Dozens Of studies world wide have proved it
possible to extend the life of a brain dead pregnant woman for
several weeks of months until she delivered a healthy child. This
proves beyond doubt that all organs and systems in the body of such
mother are functioning satisfactorily so as to ensure the safety of
the progress of pregnancy until the proposed date of delivery.
Why
do transplantation proponents insist upon the imminent death of brain
dead patients?
This
claim only shows how desperate those proponents are to harvest the
organs of such patients as soon as possible giving them no real
chance for improvement or recovery. This explains why the different
transplantation protocols agree upon the early retrieval of organs
from such patients as soon as possible, as soon as they are
pronounced brain dead (only after 24 hours in the Harvard criteria,
down to 12 hours in the Minnesota protocol and cut down to Six hours
in most protocols nowadays as the Saudi protocol for example).
NEUROLOGY
1998; 51:1538-1545
01998
American Academy of Neurology
Chronic
"brain death".
Meta-analysis
and conceptual consequences
D. Alan Shewmon,
MD
From
the Department of Pediatrics, Division of Neurology, UCLA Medical
School, Los Angeles, CA.
Address
correspondence and reprint requests to D. Alan Shewmon,
MD, Department of Pediatrics, Division of Neurology, UCLA Medical Center,
MDCC 22-474, and Box
951752, Los Angeles, CA 90095-1752.
Objective:
One rationale for equating "brain death" (BD) with death is
that it reduces the body to a mere collection of organs, as evidenced
by purported imminence of asystole despite
maximal therapy. To test this hypothesis, cases of prolonged survival
were collected and examined for factors influencing survival
capacity.
Methods:
Formal diagnosis of BD with survival of 1 week or longer. More than
12,200 sources yielded approximately 175 cases meeting selection
criteria; 56 had sufficient information for meta-analysis. Diagnosis
was judged reliable if standard criteria were described or physicians
made formal declarations. Data were analyzed by means of Kaplan-Meier
curves, with treatment withdrawals as "censored" data,
compared by log-rank test.
Results:
Survival probability over time
decreased exponentially in two phases, with initial half-life of 2 to
3 months, followed at 1 year by slow decline to more than 14 years. Survival capacity correlated
inversely with age. Independently, primary brain pathology was
associated with longer survival than were multisystem
etiologies. Initial hemodynamic instability
tended to resolve gradually; some patients were successfully
discharged on ventilators to nursing facilities or even to their
homes.
Conclusions:
The tendency to asystole in BD can be
transient and is attributable more to
systemic factors than to absence of brain function per se. If BD is
to be equated with death, it must be on some basis more plausible
than loss of somatic integrative unity.
Current
Debate on the Ethical Issues of Brain Death
Masahiro
Morioka
--
Proceedings of International Congress on Ethical Issues in Brain
Death and Organ Transplantation, University of Tsukuba, (2004):57-59
Dr.
Allan Shewmon showed in 1998 that the hearts of many brain dead patients kept
beating more than a week. 20 patients’ hearts kept beating for
at least two months, seven patients’ hearts for at least six months,
and the longest case was 14.5 years—this
patient became brain dead at the age of four, and his heart is still
beating now]. Most brain death laws were established before these
findings. And even now many specialists do not know this fact in Japan.
In these cases, the brain dead bodies become medically stable after
the acute stage, and this fact is contrary to the general public’s
belief about brain death.……………………………………………………
In 1995, a baby was born in a
rural area of Japan but soon became brain dead (no spontaneous
breathing, no brain stem reflexes, flat brain waves). In Japan,
we have no legal criteria of brain death for children under the age
of six. If we had had such criteria, this baby would have been
diagnosed as brain dead. Her parents believed that their brain dead
baby was still alive, and named her “Hina.”
They loved her, cared for her in the hospital, and their baby “lived”
to the age of four with a respirator, in the state of brain death.
The medical staff encouraged
the parents and celebrated Hina’s birthday
every year. Hina grew taller and weighed 13
kilograms when she was one year old. When Hina
“died” at age four, the parents slept with her cold body, and felt
happiness recalling the past four years. If the doctors had declared
death and organs had been removed, the parents would have never
experienced these four years with Hina.
|









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}